Home › Skin, hair and nail changes
Skin, hair and nail changes
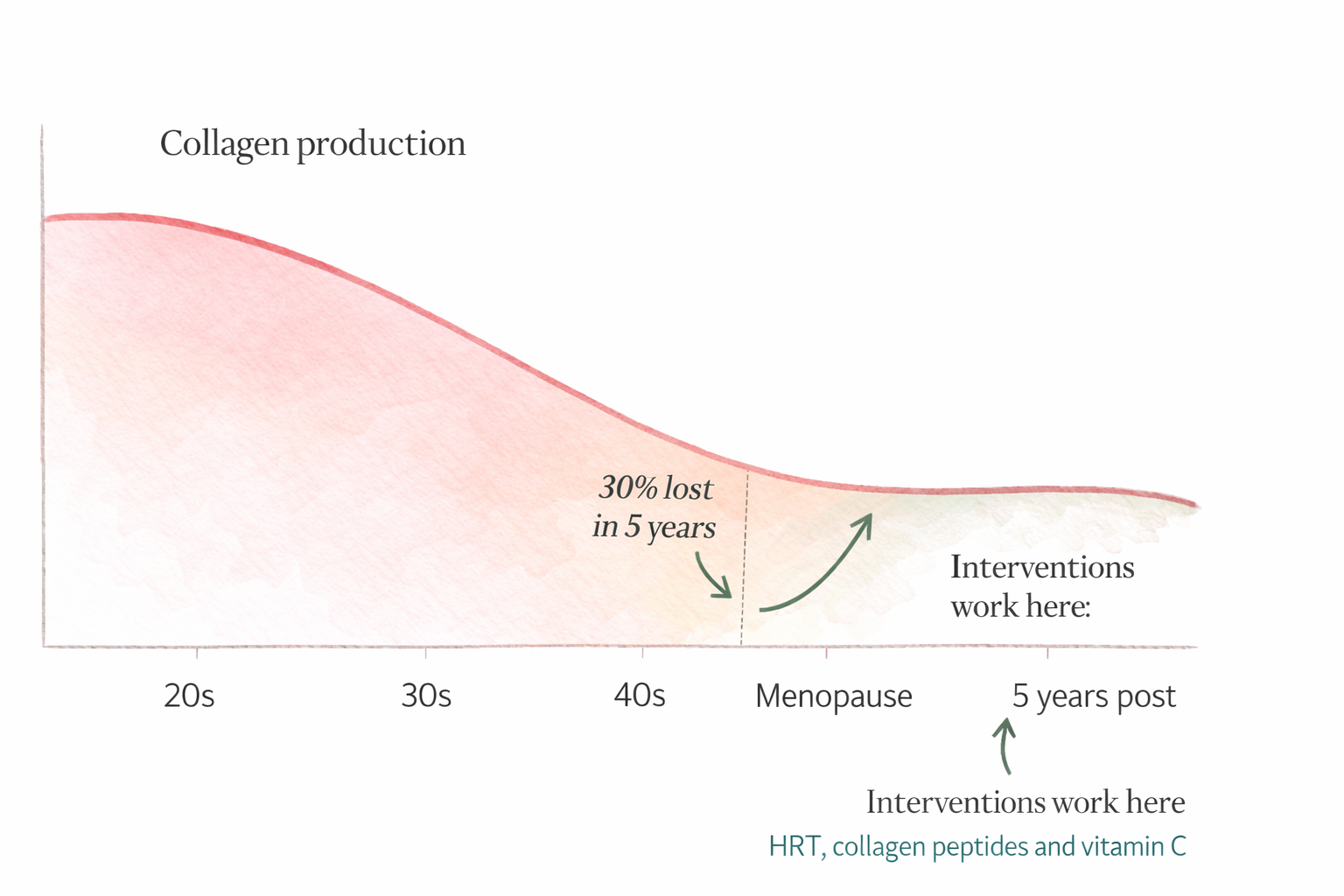
Collagen production falls by 30% in the first five years after menopause. Skin thins, hair follicles miniaturise, nails become brittle. These are real physiological changes driven by estrogen decline — not vanity, not ageing gracefully, not something to accept without understanding.

Rose
"Hair thinning was the change that hit me hardest emotionally. I was prepared for hot flashes. I was not prepared to watch my hair change. What helped was understanding that this is hormonal — not permanent damage to who I am — and finding the interventions that actually work."
Key takeaways
✓Collagen loss is fastest in the first five years after menopause — starting interventions early makes a significant difference
✓HRT has the strongest evidence for slowing skin collagen loss — it is a legitimate medical reason to consider it alongside vasomotor symptoms
✓Before attributing hair thinning to menopause, check ferritin (optimal 70-100 ng/mL), thyroid, zinc, and vitamin D — all common and treatable causes
✓Minoxidil 5% has the strongest evidence for female pattern hair loss — it requires consistent use and is maintained long-term
✓Low ferritin causes significant hair shedding even when technically within the standard lab range — optimal is higher than most labs flag as abnormal
✓Sun protection is the single most evidence-backed skin intervention — more impactful than any topical product or supplement
What is happening and why
🌿
Skin changes
Estrogen stimulates collagen and elastin production and supports oil gland function. Its decline causes skin to thin, dry, and lose elasticity. The 30% collagen loss in the first 5 postmenopausal years is the fastest rate in a womans lifetime.
💇
Hair thinning
Estrogen prolongs the hair growth phase. As estrogen falls and testosterone becomes relatively dominant, hair follicles in genetically sensitive women miniaturise — producing finer, shorter hair. Diffuse thinning at the crown is the classic pattern.
💅
Nail changes
Nails become brittle, peel, and grow more slowly. The same hormonal changes that affect skin collagen affect nail matrix cells. Low ferritin and thyroid dysfunction — both common at menopause — worsen nail health significantly.
What actually helps — skin
Collagen peptides
Mixed evidence
Hydrolysed collagen peptides provide glycine and proline — the amino acids the body uses to build collagen. Multiple RCTs show improved skin hydration, elasticity, and density with 10-15g daily over 8-12 weeks. The question of whether oral collagen reaches skin tissue is settled in favour of yes — it reaches the dermis. The question of how much improvement to expect is still being studied.
Practical
10-15g daily mixed in a drink. Bovine and marine collagen both have evidence. Takes 8-12 weeks to notice results. Vitamin C taken alongside supports collagen synthesis.
HRT — the most evidence-backed skin intervention
Strong evidence
HRT significantly reduces the rate of skin collagen loss at menopause. Studies show that women on HRT retain significantly more skin collagen than those not on it — particularly in the first 5 years after menopause when loss is fastest. Topical estrogen applied directly to facial skin has additional evidence for local collagen support.
Practical
Discuss with a menopause-literate doctor. The skin benefits of HRT are a genuine additional reason to consider it alongside vasomotor symptom relief.
Vitamin C
Strong evidence
Vitamin C is essential for collagen synthesis — it is a required cofactor for the enzymes that cross-link collagen fibres. Without adequate vitamin C, the body cannot build collagen regardless of how much collagen precursor is available. Also a direct antioxidant that reduces oxidative skin damage.
Practical
500-1000mg daily. Buffered forms are gentler at higher doses. Take alongside collagen peptides.
Sun protection
Strong evidence
UV radiation is the single largest accelerator of skin collagen loss and ageing — far exceeding the contribution of menopause itself. Daily SPF 30+ is the most evidence-backed skin intervention available regardless of age or hormonal status.
Practical
Daily SPF 30+ on face and hands. Reapply every 2 hours in sun exposure. Physical (zinc oxide, titanium dioxide) or chemical — both work.
What actually helps — hair
Rule out other causes first
Before attributing hair thinning solely to menopause, check: ferritin (low ferritin causes significant hair shedding even within standard range — optimal is 70-100 ng/mL), thyroid function (full panel including antibodies), zinc levels, and vitamin D. All are common and treatable causes of hair loss that are frequently missed at menopause.
Optimise ferritin
Strong evidence
Low ferritin is one of the most common and most treatable causes of hair loss — and one of the most frequently missed because a ferritin of 22 is technically within range. For hair health, ferritin should be above 70 ng/mL. Iron supplementation combined with vitamin C produces the most significant improvement.
Practical
Ask specifically for ferritin — not just haemoglobin or serum iron. Iron bisglycinate is the best-tolerated form. Take with vitamin C. Retest at 3 months.
Minoxidil (topical)
Strong evidence
The most evidence-backed topical treatment for female pattern hair loss. Available without prescription. Prolongs the hair growth phase and stimulates miniaturised follicles. Takes 4-6 months of consistent use to see results. Needs to be maintained — hair loss returns on stopping.
Practical
2% or 5% minoxidil solution or foam applied to the scalp. The 5% has more evidence for women. Apply to dry scalp once or twice daily consistently.
Low-level laser therapy (LLLT)
Mixed evidence
Laser caps and combs that emit low-level red light to scalp tissue. Growing evidence for stimulating hair follicle activity. More expensive than topical options but well-tolerated with no systemic effects. Best evidence is for androgenic alopecia which is what menopausal hair loss typically is.
Practical
FDA-cleared LLLT devices are available for home use. Requires consistent use 3 times per week. Give it 6 months before assessing.
HRT and testosterone
Mixed evidence
HRT helps some women with menopausal hair thinning by maintaining estrogenic support to hair follicles. Low-dose testosterone therapy has evidence for hair density improvement in women with very low testosterone — which is common at menopause. Discuss with a menopause specialist.
Practical
Raise hair thinning specifically in any HRT or testosterone discussion with your doctor. It is a legitimate clinical indication.
Nails
What helps brittle nails at menopause
• Biotin (vitamin B7) — 2.5mg daily has evidence for nail thickness and reduced splitting. Give it 6 months.
• Silica — supports collagen matrix in nail tissue. Orthosilicic acid is the most bioavailable form.
• Iron optimisation — brittle nails are a classic sign of iron deficiency. Check ferritin.
• Thyroid optimisation — brittle nails improve significantly when thyroid is properly treated.
• Hyaluronic acid — supports hydration of nail bed tissue.
• Avoid prolonged water exposure and harsh chemical contact — accelerates nail damage at any age.
Rose on this
"These changes are real. They deserve real solutions — not being told to accept ageing gracefully. Collagen peptides, optimising ferritin and thyroid, protecting from UV, and discussing HRT are all legitimate evidence-based responses. You are not being vain. You are asking for the information and the options."
From Rose
"What I found most helpful was understanding that skin and hair changes are not separate from the hormonal picture — they are part of it. Addressing the underlying hormonal and nutritional factors does more for skin and hair than any topical product. Start with ferritin, thyroid, vitamin D, and protein. The rest builds on that foundation."
What we do not know yet
?The optimal dose of collagen peptides for menopausal skin specifically — studies use 10-15g but the minimum effective dose and whether marine vs bovine differs meaningfully is not yet settled
?Whether topical estrogen applied to facial skin produces clinically meaningful collagen benefits beyond systemic HRT — early evidence is promising but trial sizes are small
?How much of menopausal hair thinning is reversible with hormonal treatment vs how much represents permanent follicle miniaturisation — this varies significantly between individuals
?The long-term safety and efficacy profile of oral minoxidil in women — the topical form is well-established but the oral version is increasingly used off-label with less long-term data
Related pages
Hair loss — symptom page ›
Collagen peptides — supplement page ›
Understanding your lab results — check ferritin and thyroid ›
Exercise — resistance training supports skin collagen ›
Written by
Rose
Living through perimenopause · Researcher · Founded rosemyfriend.com
Research basis
PubMed · Cochrane reviews · NICE guidelines · British Menopause Society · The Menopause Society
Read methodology →
Last updated
March 2026
Rose provides evidence-graded educational information — not medical advice. Always discuss health decisions with a qualified healthcare provider. Full disclaimer · About Rose